每到夏天就要去海邊啊!但去海邊就要面臨很多問題,除了會不會長痘痘、毛怎麼除以外,其中一個很麻煩的就是橘皮……人生已經夠難了,為什麼還要有橘皮!!!

根據統計,有 85% 的女性朋友可能有橘皮的困擾。但這件事情可能很多朋友不太知道原因,希望這篇文章可以給各位帶來一些新的知識,也避免在這上面花太多冤枉錢!
重點摘要
橘皮是一個多層次、多因素的症狀,因此沒有「單一最佳解法」。如果看到有什麼產品宣稱多有效,笑一笑就好。這麼有效就不會一堆人橘皮了。預防絕對遠勝於治療。這篇可看到實證有意義的預防方式,以及治療介紹。但即便是手術,也未必能得到非常滿意的解決!
橘皮是什麼?

首先一定要進行名詞解釋!先看看這張切面圖。橘皮組織(cellulite),是指皮下脂肪有些突出物突出到真皮,身體局部的脂肪厚度和彈性不同,導致皮膚表面凹凸不平,就像橘子表皮般。 而好發的位置,就是大腿、臀部、腰、腹等不易運動到的地方。多數不嚴重的橘皮平常不會被看到,但是在一些動作例如穿短褲坐上椅子的時候,可能就會不小心跑出來見人了…
橘皮的產生
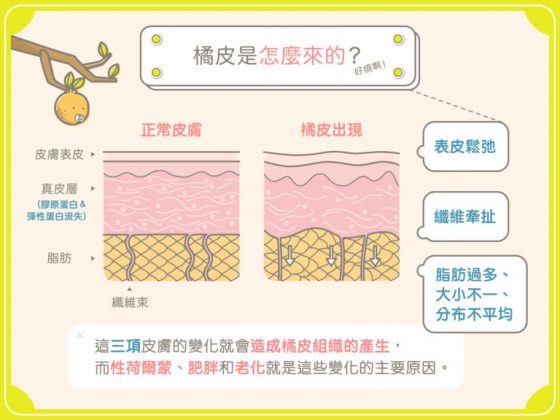
看上面這張圖。造成表面這樣的凹凸不平有許多因素,請大家看看上面這張圖。皮膚基本上分為表皮層、真皮層,然後在真皮層底下有皮下脂肪。
橘皮組織的成因通常主要是因為以下三個原因造成:
1.表皮鬆弛
2.真皮層膠原蛋白流失
3.纖維素拉扯,加上脂肪組織分佈不均、過多,導致凹凸不平
這三項皮膚的變化都會造成橘皮的產生,而性賀爾蒙、肥胖以及老化就是這些變化的主要原因。
橘皮男女大不同!?

接下來要講一個非常殘酷,只能無語問蒼天的事實。大家有沒有發現橘皮幾乎都是女生在講,google 圖片也都是女生的腿,難道男生就沒有橘皮嗎?其實,男生不是完全不會有橘皮,而是比起女生來說非常不容易產生。主要原因,就是「纖維束」的方向。
從圖可以看到女生的脂肪比較不平整,另外纖維束的走向比較垂直,把真皮組織往下拉的纖維束,會讓脂肪表面變不平整。而斜的纖維束走向讓男生不像女生容易有凹凸不平的皮膚,至於為什麼會這樣,醫生和科學家們還在研究,應該跟性賀爾蒙有關。這就是男生比較不會有橘皮,而青春期後85%的女性都會有這樣的困擾!
以下開放女性同胞們哭泣十秒鐘。男性同胞請默哀。
三、二、一。好,擦乾眼淚,我們繼續上課QQ
橘皮分級

橘皮的嚴重程度是有分級的!
0 級:沒有明顯的橘皮與位置。隨著捏皮膚,也沒有出現的橘皮組織。
1 級:站立時沒有贅肉,但捏大腿的皮膚,就會看到有點像床墊外觀的皮膚。
2 級:有明顯的橘皮,特別是站立時,但躺下時並不明顯。
3 級:無論站立或躺下,都有明顯的橘皮。
如果是 0-1 級,恭喜你,好好預防。
如果是 2-3 級,那就,嗯,加油,這條路不好走…
橘皮的治療
接下來還是要講一些治療方式。
按摩霜
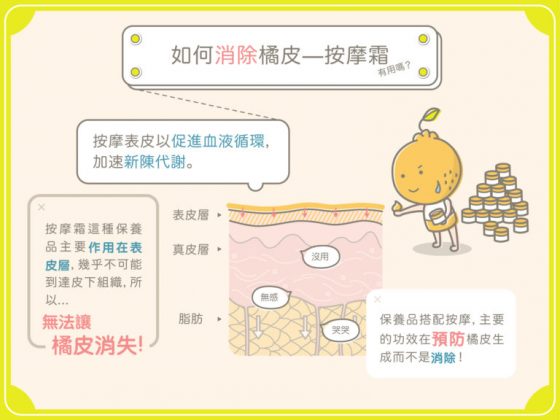
大家應該都聽過市面上各種說含什麼什麼成分的按摩霜。基本上,按摩表皮以促進血液循環,加速新陳代謝,沒啥大問題。但按摩霜這種保養品主要作用在表皮層,幾乎不可能到達皮下組織,所以沒辦法讓橘皮真正消失。保養品搭配按摩,主要的功效在預防橘皮生成而不是消除!
除了功效上的疑慮外,成分也是個大問題,許多按摩霜的主成分包含辣椒、薄荷、咖啡因等成分,可以短效促進局部代謝、排水,但是這些成分難以作用到皮下脂肪層,基本上無法真的消除脂肪!
脈衝光

脈衝光基本上是利用一系列不同波長的光刺激不同的組織,促進真皮層增生膠原蛋白,讓表皮緊實,進而改善表面的凹凸不平。他作用的層次主要在表皮層與真皮層。至於脂肪層,就比較有困難啦~
電波拉皮

電波會產生熱能,刺激真皮層增生膠原蛋白,因此可能可以改善橘皮。另外在醫師的評估下,某些電波可以作用到淺層的脂肪。因此作用層次比起脈衝光要來得深一些。
抽脂

最後也是最刺激的來了,抽脂會抽出身體不正常堆積的脂肪,另外也有醫師認為纖維束被打斷能讓表皮變平整。
基本上脂肪細胞一旦形成就不太會消失,只會變大或是變小,除非是用破壞性的方式把脂肪細胞移除,不然你變胖變瘦,大多只是細胞變小變大而已。
預防橘皮

大家上完剛才的解剖課,應該有基本的概念了。因為橘皮的成因複雜,影響橘皮的因素很多,且每個人的狀況不同。
因此,
沒有單一最佳的解決方法!
沒有單一最佳的解決方法!
沒有單一最佳的解決方法!
很重要一定要說三次!!!
如果你聽誰說,他可以「保證」把你橘皮處理到好的,把這篇文章給他看,然後叫他去教室外面跪著!!!真的那麼強,阿我們這些醫生都去死一死就好了啊~~~
所以養成好習慣好好預防很重要喔~
以下是幾個可以請大家跟著做的:

1.維持標準體重:橘皮組織會因為脂肪囤積而產生,因此體脂維持在正常的範圍就較不會有橘皮生成。
2.多做下肢運動:避免大腿、臀部囤積脂肪。
3.延緩皮膚老化:減少真皮層中的彈力纖維蛋白流失的速度,必須注重防曬、皮膚保濕,才能保持肌膚彈性。
多運動,也會改善肌肉跟脂肪的組成比例,大家千萬別久坐喔!沒事可以多上哥的課,常常會有去教室外面深蹲的機會,有益身心健康!
常見Q&A
Q:有些按摩霜說含有生長因子,可以撫平橘皮,到底有沒有效?
A:阿他生長因子是什麼?哪種生長因子?作用在哪個層次?這麼會撫平怎麼不來撫平我被噓內心的創傷 QQ 叫他給我出去外面跪!!!不要忘記解剖學,橘皮是多層次的問題,沒有單一最佳解!
Q:努力去角質對橘皮有沒有幫助?
A:角質頂多在表皮的層次,跟皮膚彈性也沒關係。至於底下真皮層跟脂肪,去角質根本無法處理到啊!!!!問這個問題的同學,先出去蹲十分鐘再進來。
Q:是不是真的抽脂就可以改善橘皮問題?
A:不一定。要看你產生橘皮的問題在哪個層次。如果表皮還算緊,真皮層流失不嚴重,只是脂肪很多的狀態,那多數會有還算明顯的效果。但如果表皮已經很鬆,那可能還要搭配其他手術,把多餘的皮去掉,不然會一堆皮掛在那很醜…
橘皮是非常多人的煩惱,你隨便 google 就會看到一堆產品,但拜託大家,看懂生理解剖結構之後,能夠自己想想, 到底哪些商品是可能真的有效,哪些是無效又花錢的。祝福大家在對抗橘皮的路上,都別走錯路,花錯錢啦!
編按:愛美是每個人的天性,不過對你而言光是看滿架的化妝品、保養品,各種醫美產品就令你眼花撩亂,更別說還有玻尿酸、膠原蛋白、類固醇這些有聽沒有懂的名詞來搗亂嗎?如果你想要聰明的美,不想要被各種不實廣告唬得團團轉,那麼泛科學這位合作夥伴 MedPartner 美的好朋友,就是你我的好朋友。
本文轉載自MedPartner 美的好朋友