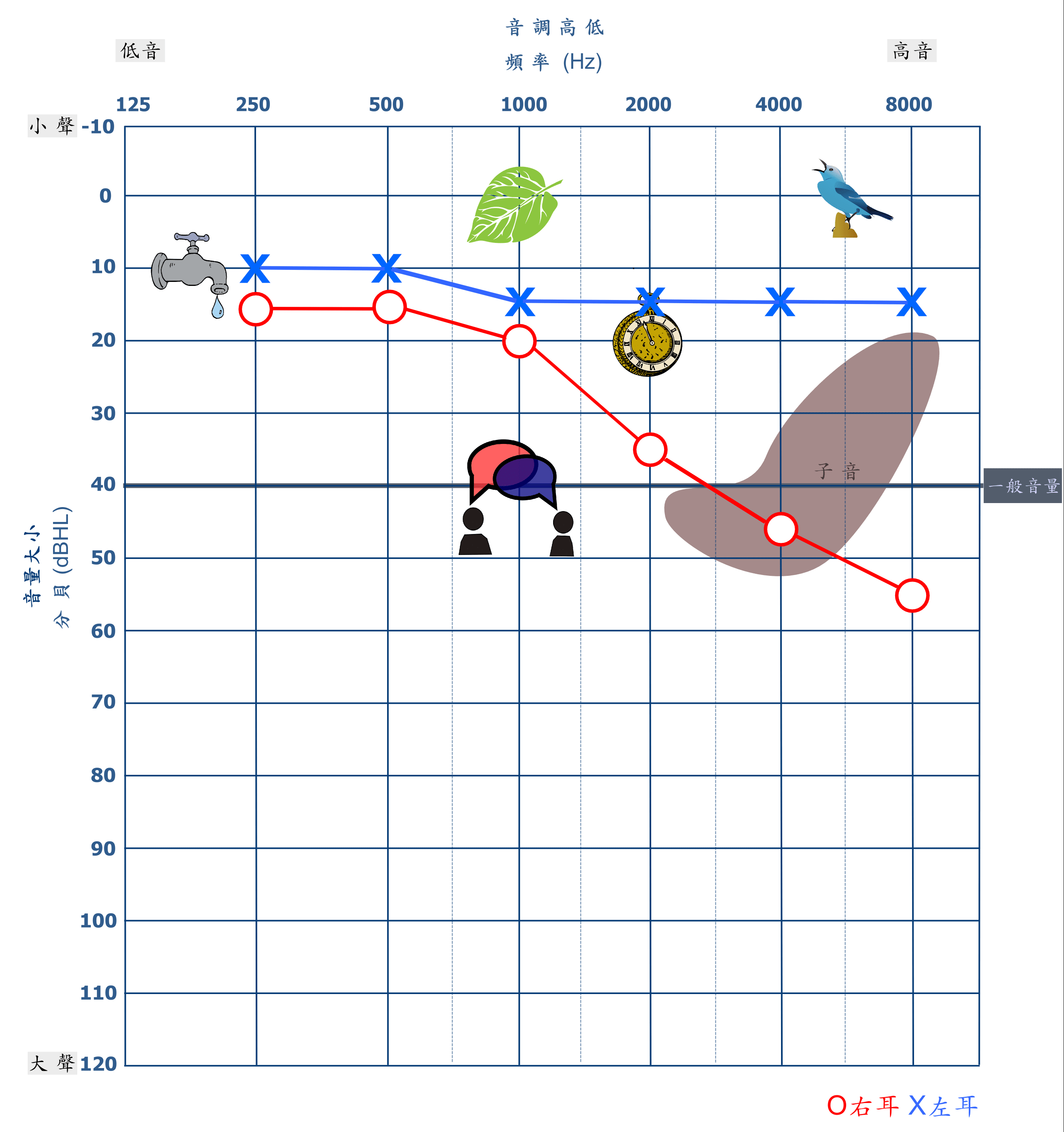
一般來說,一邊耳朵聽力正常,另一邊耳朵的聽力在 500 Hz、1,000 Hz、2,000 Hz三個頻率的平均聽力閾值(也就是能夠聽到的最小音量)大於 20 dB HL;或是在 2,000 Hz 以上至少 2 個頻率的聽力閾值大於 25 dB HL,就可以說是「單側聽力損失」(Centers for Disease Control and Prevention, 2005; Eichwald& Gabbard, 2008)。
單耳聽損程度不論是輕至極重度皆稱為單側聽損。但其中約有 59%單側聽損者的聽損程度落於輕度至中度之間 (Fitzpatrick et al., 2014),也就是大約落在 26-55 dB HL這個範圍。下圖為一單側聽力損失聽力圖示例。
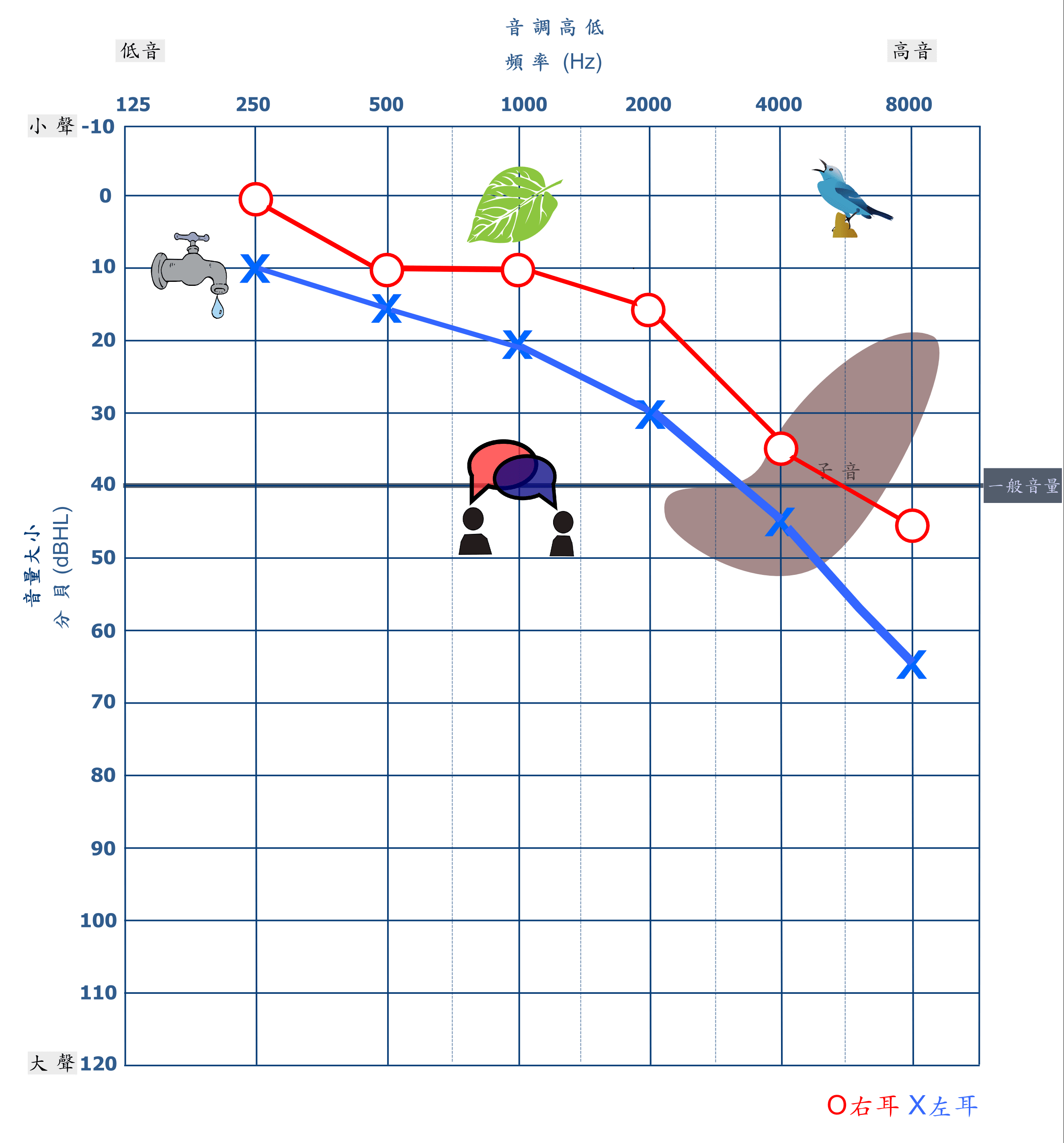
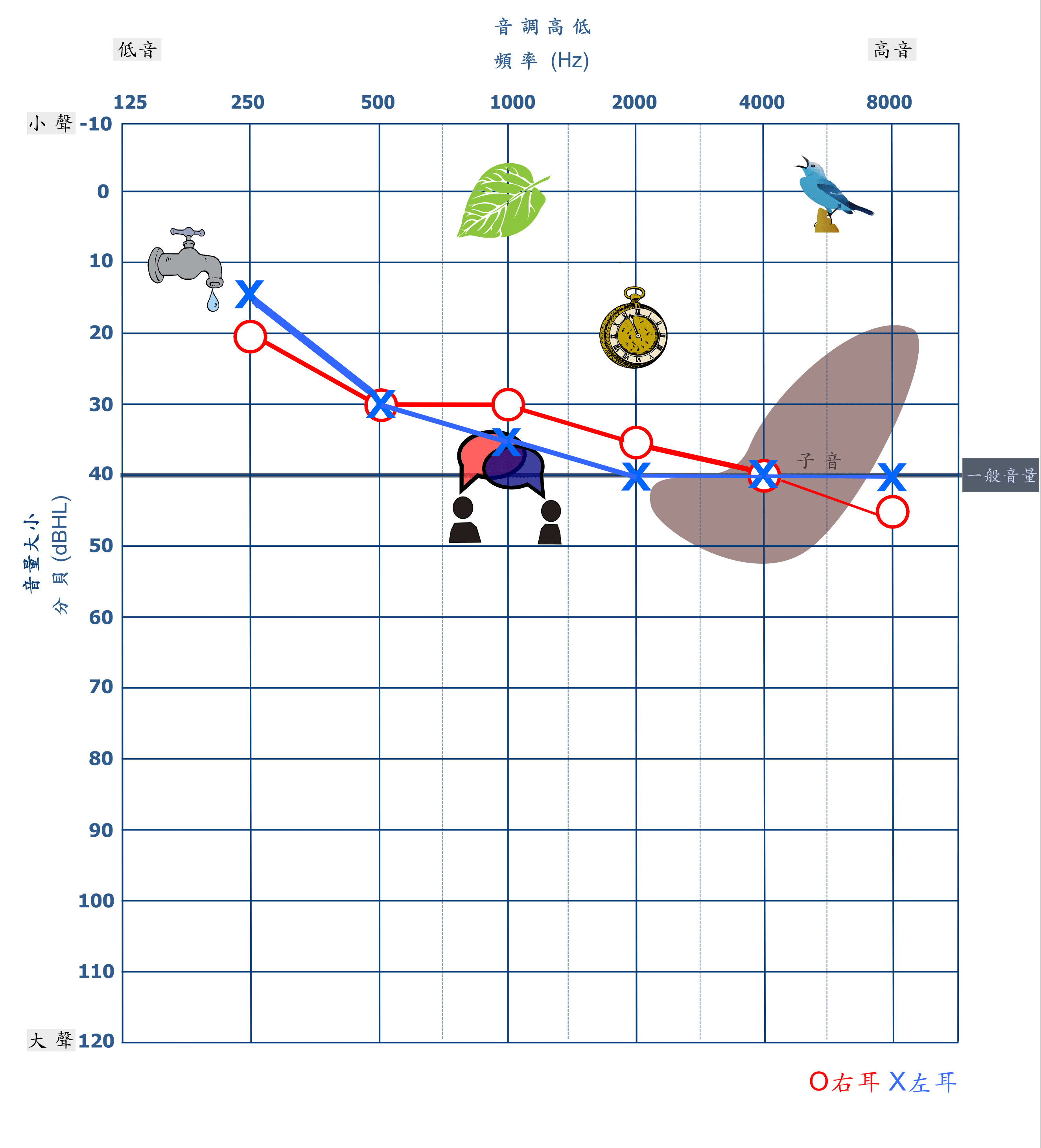
我們可以說這樣的小美人魚是「輕型聽力損失」,輕型聽損指的是兩側耳朵的平均聽力閾值介於 20-40 dB HL(Educational Audiology Association, 2017),也就是介於國際標準畫分的極輕度與輕度聽損間。下圖為一輕型聽力損失聽力圖示例。
和高頻聽損者所遭遇的情況類似,輕型聽損者是可以聽到聲音的。以 40 dB HL聽損為例,由於無法接收到 40 dB HL以下的聲音,而一般對話的語音音量則多數分佈於這個區域,沒有聽到這些語音會導致部份語音訊息流失,也更容易在對話中會錯意,所以在吵雜環境及遠距離對話中,輕型聽損者也更容易遺漏訊息(Anderson, K. & Matkin, N., 1991, 2007 revised)。
-----廣告,請繼續往下閱讀-----
正因為如此,輕型聽損的小美人魚除了白白錯失了跟王子共舞的機會,也可能會讓王子誤會小美人魚是高傲或是不想跟王子講話、跳舞,長久下來也難以拉近彼此的距離,甚至出現社交困難(Anderson, K. & Matkin, N., 1991, 2007 revised)。
發現有微聽損,該怎麼做?
當發現聽力損失時,聽覺輔具(助聽器、FM系統、助聽器+FM系統)往往是最優先被考慮的介入方式。像是高頻聽損及輕型聽損,過去已有許多文獻支持輔具使用的效果(Yoshinaga- Itano, 2003; Nina J. et al., 2017)。
此時大腦一方面需要費力處理模糊的語音訊息,同時另一方面還需費力地理解課程內容。這樣的情境對於成年人來說尚且已經構成負擔,對於微聽損兒童來說,在課堂上因為需要費力聽清楚上課時老師的每個語音,同時也要理解上課的內容,他們將會更加疲累且壓力更大。(McFadden and Pittman 2008; Dokovic et al, 2014)。
這樣的擔憂不是沒有道理的,英國的教師甚至發現重至極重度聽損孩子的課業表現反而比輕至中度聽損孩子還好(The Ear Foundation, 2015),微聽損兒童健康相關生活品質也低於重度聽損的兒童(Wake et al., 2004),更有研究顯示微聽損兒童的自信心低於聽力損失嚴重的兒童(Keilmann et al., 2007)。
這些發現在在顯示,聽損程度較重的孩子可能因為較早使用輔具且進行早療(Walker et al。2015),因而得到較多資源支持,但聽損程度較輕的孩子需求則常常被忽略。青少年的研究也指出,相較於重度聽損的青少年,微聽損的青少年可能更容易感到焦慮(Van Gent et al。2011)
正因如此,我們必須意識到,即使是輕型的雙側和單側聽損也可能增加適應不良的風險 (Tharpe 2008, Winiger et al. 2016)。所以,微聽損者可以尋求聽語專業人員給予適當的衛教建議,如:追蹤頻率、日常觀察技巧或是說明什麼狀況需要就醫檢查,以便及時得到專業協助。
Anderson, U. M. (1967). The incidence and significance of high-frequency deafness in children. American Journal of Diseases of Children, 113(5), 560-565.
Bess, F. H., Dodd-Murphy, J., & Parker, R. A. (1998). Children with minimal sensorineural hearing loss: prevalence, educational performance, and functional status. Ear and hearing, 19(5), 339-354.
Bess, F. H., Klee, T., & Culbertson, J. L. (1986). Identification, assessment, and management of children with unilateral sensorineural hearing loss. Ear and Hearing, 7(1), 43-51.
Bess, F. H., & Tharpe, A. M. (1984). Unilateral hearing impairment in children. Pediatrics, 74(2), 206-216.
Bovo, R., Martini, A., Agnoletto, M., & Beghi, A. (1988). Auditory and academic performance of children with unilateral hearing loss. Scandinavian Audiology.
Đoković, S., Gligorović, M., Ostojić, S., Dimić, N., Radić-Šestić, M., & Slavnić, S. (2014). Can mild bilateral sensorineural hearing loss affect developmental abilities in younger school-age children?. Journal of deaf studies and deaf education, 19(4), 484-495.
Eichwald, J., & Gabbard, S. A. (2008, May). Mild and Unilateral Hearing Loss in Children. In Seminars in Hearing(Vol. 29, No. 02, pp. 139-140). Published by Thieme Medical Publishers.
English, K., & Church, G. (1999). Unilateral hearing loss in children: an update for the 1990s. Language, Speech, and Hearing Services in Schools, 30(1), 26-31.
Fitzpatrick, E. M., Whittingham, J., & Durieux-Smith, A. (2014). Mild bilateral and unilateral hearing loss in childhood: A 20-year view of hearing characteristics, and audiologic practices before and after newborn hearing screening. Ear and hearing, 35(1), 10-18.
Keilmann, A., Limberger, A., & Mann, W. J. (2007). Psychological and physical well-being in hearing-impaired children. International Journal of Pediatric Otorhinolaryngology,71(11), 1747-1752.
Laugen, N. J., Jacobsen, K. H., Rieffe, C., & Wichstrøm, L. (2017). Social skills in preschool children with unilateral and mild bilateral hearing loss. Deafness & Education International, 19(2), 54-62.
McFadden, B., & Pittman, A. (2008). Effect of minimal hearing loss on children’s ability to multitask in quiet and in noise.Language, speech, and hearing services in schools, 39(3), 342-351.
Niskar, A. S., Kieszak, S. M., Holmes, A., Esteban, E., Rubin, C., & Brody, D. J. (1998). Prevalence of hearing loss among children 6 to 19 years of age: the Third National Health and Nutrition Examination Survey. Jama, 279(14), 1071-1075.
Tharpe, A. M. (2008). Unilateral and mild bilateral hearing loss in children: past and current perspectives. Trends in amplification,12(1), 7-15.
The Ear Foundation (2015). Experiences of young people with mild to moderate hearing loss: Views of parents and teachers. The Ear Foundation report to NDCS: Mild-moderate hearing loss in children.
Van Gent, T., Goedhart, A. W., & Treffers, P. D. (2011). Self‐concept and psychopathology in deaf adolescents: preliminary support for moderating effects of deafness‐related characteristics and peer problems. Journal of Child Psychology and Psychiatry,52(6), 720-728.
Wake, M., Hughes, E. K., Collins, C. M., & Poulakis, Z. (2004). Parent-reported health-related quality of life in children with congenital hearing loss: a population study. Ambulatory Pediatrics, 4(5), 411-417.
Walker, E. A., McCreery, R. W., Spratford, M., Oleson, J. J., Van Buren, J., Bentler, R., … & Moeller, M. P. (2015). Trends and predictors of longitudinal hearing aid use for children who are hard of hearing. Ear and hearing, 36(0 1), 38S.
Wang, P. C., Chang, Y. H., Chuang, L. J., Su, H. F., & Li, C. Y. (2011). Incidence and recurrence of acute otitis media in Taiwan’s pediatric population. Clinics, 66(3), 395-399.
Winiger, A. M., Alexander, J. M., & Diefendorf, A. O. (2016). Minimal hearing loss: From a failure-based approach to evidence-based practice. American journal of audiology, 25(3), 232-245.
Yoshinaga‐Itano, C. (2003). Early intervention after universal neonatal hearing screening: impact on outcomes. Developmental Disabilities Research Reviews, 9(4), 252-266.
{kind=link}
{kind=link}
{kind=link}
View Comments